Abbreviations
- CCOPMM: Consultative Council on Obstetric and Paediatric Mortality and Morbidity
- MCHN: Maternal and Child Health Nurses
- VVED: Victorian Virtual Emergency Department
Definitions
Abrasion - A superficial scraping injury of the body surface with or without bleeding.
Bruise/bruising - caused by bleeding under intact skin due to trauma. Bruises are common childhood injuries. Bruising is also the most common injury sustained by children who have been abused.1
Caregiver - birth parent, adoptive parent, foster parent, guardian, kinship carer, person responsible for child’s care.
Child Abuse - any act or failure to act by a caregiver that endangers a child’s physical or emotional development. It may be a single incident or pattern of care, which over time accumulates to cause harm to a child’s development or wellbeing” It can be physical, emotional, sexual, or neglect.5
Congenital dermal melanocytosis (CDM previously known as Mongolian blue spots) - flat blue/grey birth marks spots with an irregular shape that commonly appear at birth or soon after.17
Contusion - the medical term for a bruise. See ‘bruise’ definition.
Frenulum - Superior Labial Frenulum of the upper lip, is a fold of mucous membranes that connects the upper lip to the gum, which can be easily torn when the mouth is hit, or the lip is pulled/stretched.
Inferior Labial Frenulum - of the lower lip, is a fold of mucus membrane that connects the lower lip to the gum.18
Haematoma - a closed wound where blood collects and fills a space inside your body because it can’t flow or drain out.19 Usually associated with swelling e.g. “egg” on the forehead.
Infant -Typically refers to an infant from birth to 1 year of age.20
Immobile infant - an infant not yet independently rolling, crawling, bottom shuffling, pulling to stand or cruising i.e. those infants who cannot move themselves from where they are placed.21
Incision - A cutting type of injury that severs tissues in a clean and generally regular fashion.
Laceration - A tear or split in the tissues.
Other Staff - Includes allied health, early childhood professionals, student MCH nurses; MCH Leadership.
Petechiae - Red or purple, pin prick size dots red or purple in colour that are non-blanching often occurring in clusters. A pinpoint sized (0.1-2mm) haemorrhages into the skin due to acute rise in venous pressure.
TEN-4-FACESp - Torso, Ears, Neck in any child under 4 yrs, any bruising <4-6mo and Frenulum; Angle of the jaw; Cheek; Eyelid; Subconjunctival Haemorrhage.12
Sentinel injuries - a previous injury (prior to severe physical abuse) reported in the medical history that was suspicious for abuse because the infant could not cruise, or the explanation was implausible.3
Background and purpose
Purpose
- To ensure Maternal Child Health (MCH) Nurses have a clear understanding of and comply with their legislative requirements, codes of conduct, standards and processes when suspected bruising on the immobile infant is observed.
- To ensure consistency of MCH practice when a suspected bruise is observed on an immobile infant.
Background
- Infants are overrepresented in child physical abuse, this is attributed to their increased vulnerability and care needs6
- Bruising on an immobile infant raises concern about health and safety.7
- Sentinel injuries in infants are minor, visible injuries, such as bruises or intraoral injuries that are unexplained or have an implausible mechanism of injury, that raise concern for physical abuse. They are not typically serious in themselves but can be an early warning sign of potential abuse, sometimes preceding more severe injuries.8 External injuries are highly predictive for more severe maltreatment.9
- Bruising is the most common finding in child abuse.6
- Child abuse is a common cause of paediatric morbidity and mortality6
- Bruising is rare in immobile infants6 less than 1%.7
- In their systemic review of 23 studies 1951-2004, bruising was found in 17% infants who were crawling or cruising with most preschool and school aged children having bruises.7
- All staff should be aware of potential factors that contribute to and place an infant at risk of harm.10,11
- The TEN-4 clinical decision tool (Bruising to torso, ear or neck or any bruising on an infant < 4 months of age) can be used to assess possible bruising or identifying children at risk of having been physically abused.12
- Bruising and marks need to be distinguished from medical concerns such as skin lesions or bleeding disorders or Vitamin K deficiency.13-15
- It is important that clinicians are trained in identifying birth marks and proper documentation of these to avoid confusion with bruises and avoid unnecessary stress for parents.16
- When bruising is suspected it must be assessed in the context of medical, social and developmental history, explanation given and pattern of bruising.7
Assessment
History – check electronic Health Record, documentation of marks on skin (e.g. birth mark)
- Check the electronic Health Record and caregiver held child health record for documentation of birth marks already observed by MCHN or maternity service providers.22
- Check for any previous history of injuries, neglect or psychosocial risk.23
- Best practice is for MCH services to make every effort to obtain copies of all postnatal care records such as newborn assessment and discharge summary.
Suspect bruising - assume abuse or bleeding disorder
- Check for any family history of bleeding disorders.23
- Be alert for other possible injuries such as subconjunctival haemorrhage, fractures or burns.
- Look inside the mouth for signs of torn lingual or labial frenulum, or petechiae.23
Further assess the situation – including infant and parent/care giver assessment
In a conversational manner, sensitively and nonjudgmentally ask the parent if they had noticed the mark and if they know what may have caused it.21,24
Ask direct questions:
- Have you noticed this mark/bruise?
- Do you know how/when this mark/bruise occurred?
- Has the mark/bruise been reviewed by a medical practitioner/paediatrician?
- Are there any blood disorders in the family?
- Did you or someone else hurt your baby?
- Document answers verbatim, wherever possible.11,24
Consider history and explanation of the mark/bruise given by carer.
- Check plausibility and consider how the mechanism fits with the location and shape of the bruise.23
- Check the consistency or changes of history, mechanisms given or vagueness.23
- Check medications or herbal remedies given that may lead to abnormal clotting.23
- Check for any traditional remedies given such as cupping or coining.23
- Assess any psychosocial risk factors such as family violence, prior child protection involvement or criminal history.23
Perform physical assessment visit including physical check, growth, identify undocumented bruising / mark
When observing a bruise/ mark complete a detailed history, full physical examination and developmental assessment.23
- Full examination of child is required, remove all clothing and nappies. Examine carefully, including around neck and ears.23
- Record height, weight and head circumference on percentile charts.25
- Observe how the child interacts with carers and other adults.23
Observe any bruises: Note details re bruise / mark; size, shape, symmetry, colour, texture, location.7,23
- Location of the bruises - More common on bony prominences or in younger children, a T-shape zone across forehead, nose, upper lip, chin or the back of the head. Accidental bruises are less common on ear, eyes, cheek, neck, hands or genitalia. Rare for children with bleeding disorders to have bruising on ears, eyes, neck or genitalia. Ankles, wrists suggest possible ligatures.23
- Patterns and clustering - Note if the bruise resembles the shape of an implement. Linear bruises with areas between them suggest fingers. Slap marks on face are more common on left cheek due to most perpetrators are likely to be right-handed.23
- Note number of bruises - It is rare for a single injury to cause more than one bruise; simple falls, collisions or impact injuries do not result in multiple bruises. Exception is long stair falls of 10 or more steps, sports injuries or car collisions.23
- Note any petechiae - Petechiae in association with a bruise in a child without bleeding disorders is suggestive of abuse. Petechiae on upper chest or neck may be the result of severe chest compression.23
- Colour of bruises – change, but do not appear in a predictable fashion. Bruises and other similar looking skin lesions can appear differently on varying skin tones. You cannot age a bruise with the naked eye.23
Use TEN-4 FACESp clinical decision tool to assess bruising.12

A single bruise in an infant aged ≤ 4 months, is considered a Red Flag.
In children aged < 4 years
- Torso – marks caused by trauma, spanking, impact with objects. NOT idiopathic scrotal oedema, testicular torsion or torsion of an appendix testis, hydroceles, varicocele or epididymo-orchitis.
- Ears – marks or Haemotympanum caused by impact (e.g. slapping), lacerations caused by traction. NOT ‘tin ear syndrome’ - ipsilateral cerebral oedema.
- Neck – marks caused by trauma, strangulation. Also check for petechiae above/beyond the ligature / venous occlusion. NOT self-infliction (e.g. scratches), marks from clothing.
- Frenulum – labial injury / tear (laceration), lingual frenulum trauma (laceration, laser, incision), sublingual trauma. (haematoma)
- Angle of the jaw – marks over the angle of the jaw.
- Cheek - soft/fleshy part
- Eyelids
- Subconjunctivae / Sclera (white of eyes)
- Patterned (also petechiae)
Management
- Where appropriate and safe to do so, discuss with parent the need for further assessment.
- If the child is in imminent danger, call 000, otherwise proceed as below.
- Suggest a review, as these marks can be due to medical conditions that could be very serious, such as bleeding disorders.23
- Advise parents you will contact the Emergency Dept, Urgent Care Centre, Victorian Virtual Emergency Department or GP that they will be bringing the infant in for assessment/review.26
- Refer for immediate medical review and/or differential diagnosis to Emergency Dept, Urgent Care Centre, Victorian Virtual Emergency Department or GP with paediatric speciality as appropriate for your service location.21
- Notify the Emergency Department, Urgent Care Centre, Victorian Virtual Emergency Department or GP that the child has been referred for assessment of bruising / marking and follow up to ensure this has occurred.10,11,24
- Ensure safety of the child – discuss risk assessment with MCH Leadership to assess the risk and protective factors so they can provide guidance and support on the management plan.10,11
- To make a report to child protection a person needs to have formed a reasonable belief that a child has suffered or is likely to suffer significant harm as a result of abuse or neglect and that their parent has not protected or is unlikely to protect the child from harm of that type. 21,23
- Working in partnership with families to devise the management plan, while also informing them of the mandatory reporting obligation, if safe to do so.
- Ensure follow up with the family, medical team and Child Protection (if involved) about the outcome after a medical review.26
Documentation
- Record details of your observations and actions carefully in MCH electronic health record, noting location, size, shape, symmetry, colour, texture of bruise/mark.10
- Include referrals made and who you have spoken to (obtain name & contact details) e.g. hospital, MCH Coordinator, Child Protection. (If involved)
- Place flags/alerts on MCH electronic health record and upload copies of referral form and ‘Baby Body Check’ diagrams to infant MCH electronic health record file.24
- Document all actions in electronic health record, including follow up.
Referrals
What to refer
Bruising always requires referral and follow-up to ensure that referral has been actioned and appropriate information has been shared.27
Use the TEN 4 FACESp guidelines to guide assessment and support referral.
When and who to refer to
- Refer for immediate medical review to Emergency dept, Urgent care centre, Victorian Virtual Emergency Department or GP with paediatric speciality, as appropriate for the service location.21
- Consult with your Team Leader / MCH Coordinator to discuss the risk and protective factors for them to provide guidance and support on the management plan.10,11,27
- make a mandatory report to Child Protection if a belief is formed that the child has been or is being physically harmed.
Ensure the management plan has been communicated to the family, where safe to do so.
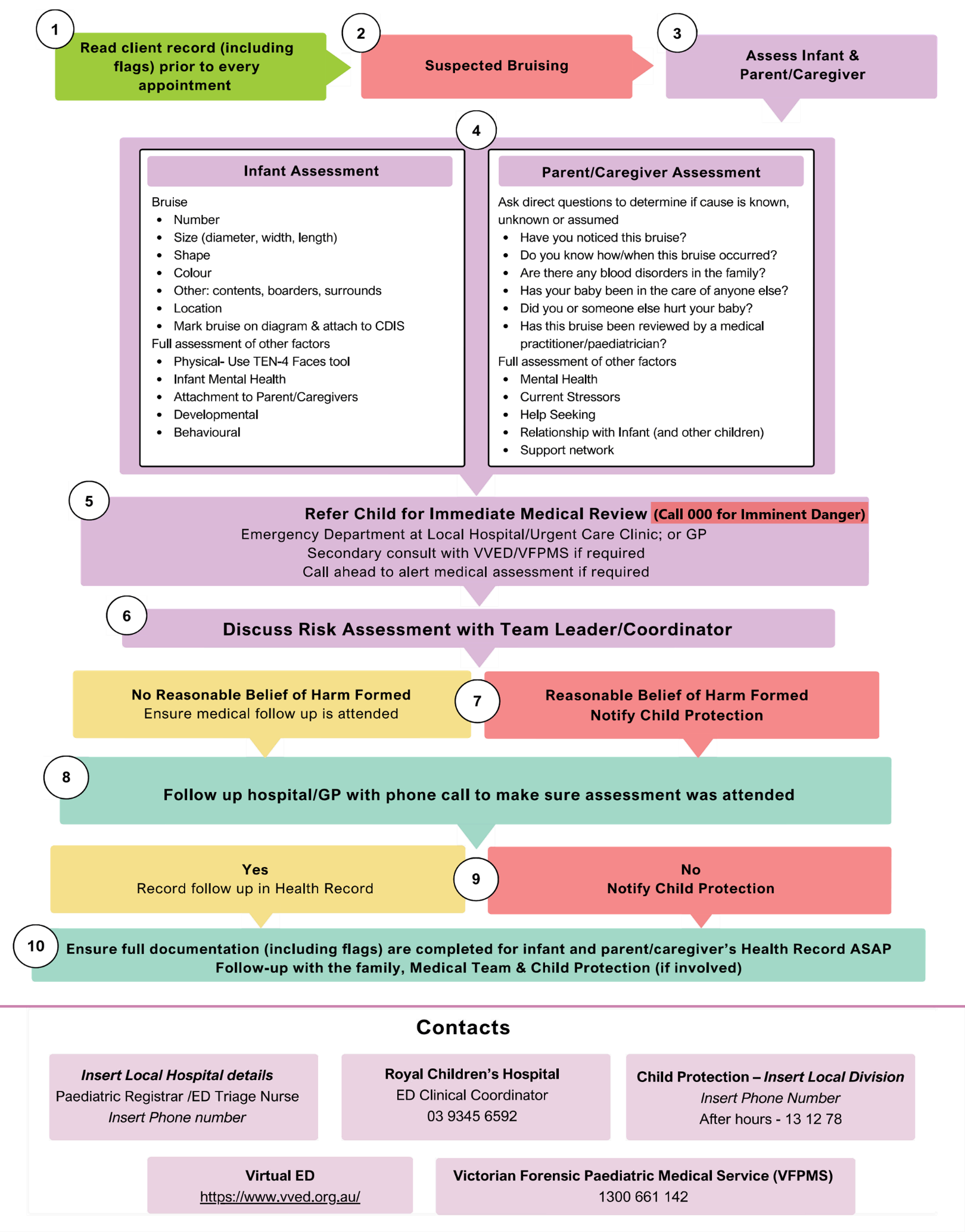
Flowchart – Bruising on the immobile infant
Additional information for health professionals
Bruising | Royal Children's Hospital
Clinical Practice Guidelines : Child abuse | Royal Children's Hospital
Victorian Forensic Paediatric Medical Service : About VFPMS | Royal Children's Hospital
Identifying signs of child abuse | Victorian Government
MCH Practice | Municipal Association of Victoria
Additional information for families
Fact sheets - Congenital dermal melanocytosis | Royal Children’s Hospital
Bruises and bruising | Raising Children Network
Maternal Child Health Services | Better Health Channel
References
1. Victorian Forensic Paediatric Medical Service (VFPMS). Guideline: Forensic investigation of bruising [Internet]. 2025 [cited 2025 Aug 4]. Available from: https://www.rch.org.au/vfpms/guidelines/Bruising/
2. Feldman KW, Tayama TM, Strickler LE, Johnson LA, Kolhatkar G, DeRidder CA, Matthews DC, Sidbury R, Taylor JA. A prospective study of the causes of bruises in premobile infants. Pediatr Emerg Care. 2020 Feb;36(2):e43–9. https://doi.org/10.1097/PEC.0000000000001311
3. Sheets, L., Leach, M., Koszewski, I., Lessmeir, A. Nugent, M. & Simpson, P. (2013). Sentinel injuries in infants evaluated for child physical abuse. Pediatrics Apr;131(4):701-7. doi: 10.1542/peds.2012-2780.
4. Cho, N. & Koti, A. (2024) Identifying inflicted Injuries in infants and young children. Seminars in Pediatric Neurology, 50 DOI.org/10.1016/j.spen.2024.1011.38
5. Dept of Health. Maternal and Child Health Service Guidelines [Internet]. Melbourne (AU): Victorian Government; 2021 [cited 2025 Aug 5]. Available from: https://www.health.vic.gov.au/publications/maternal-and-child-health-service-guidelines
6. Cho N, Koti AS. Identifying inflicted injuries in infants and young children. Semin Pediatr Neurol. 2024;50:101138. https://doi.org/10.1016/j.spen.2024.101138
7. Maguire S, Mann M, Silbert J, Kemp A. Are there patterns of bruising in childhood which are diagnostic or suggestive of abuse? A systematic review. Arch Dis Child. 2005;90(2):182–6. doi:10.1136/adc.2003.044065
8. An L, Wang C. Ear bruising in a newborn. Clin Pediatr (Phila). 2024;63(4):576–9.
9. Feld K, Ricken T, Feld D, Helmus J, Hahnemann M, Schenkl S, et al. Fractures and skin lesions in pediatric abusive head trauma: a forensic multi-center study. Int J Legal Med. 2021;135(6):2281–90. Available from: Springer PDF
10. City of Whittlesea. Maternal and Child Health. Marks on an Immobile Infant. Policy and Procedure. 2024
11. City of Frankston. Bruising on a Non-mobile Infant. Clinical Procedure. 2023
12. Pierce MC, Kaczor K, Lorenz DJ, et al. Validation of a clinical decision rule to predict abuse in young children based on bruising characteristics. JAMA Netw Open. 2021;4(4):e215832. doi:10.1001/jamanetworkopen.2021.5832
13. Hostman A, Southwell J, Danchin M, Smith A. Vascular naevi can mimic bruising in an infant. J Paediatr Child Health. 2022;58(3):524–5.
14. Bui J, Naing P, Cathers P, Ahmad M, Cohen B. Chest wall bruising from 5-point car seat harness as a mimicker of child abuse. Pediatr Dermatol. 2023;41:718–21.
15. Holley S, Detterman C, Thayer S. An infant with bruising and lethargy. J Nurse Pract. 2021;17:634–7.
16. Harrison S, Saran S. Suspected non-accidental injuries: which blood tests to do? Arch Dis Child. 2021;106(Suppl 1):A154–5.
17. Royal Children’s Hospital (RCH). Kids info fact sheet: Congenital dermal melanocytosis [Internet]. [cited 2025 Aug 5]. Available from: https://www.rch.org.au/kidsinfo/fact_sheets/Congenital_dermal_melanocytosis/
18. Fox S. Frenulum tear. Pediatric EM Morsels [Internet]. 2017 Mar 24 [cited 2025 Aug 5]. Available from: https://pedemmorsels.com/frenulum-tear/
19. Cleveland Clinic. Diseases: Hematoma [Internet]. [cited 2025 Aug 5]. Available from: https://my.clevelandclinic.org/health/diseases/hematoma
20. World Health Organization Western Pacific. Newborn health [Internet]. [cited 2025 Aug 5]. Available from: https://www.who.int/westernpacific/health-topics/newborn-health?utm_source=chatgpt.com#tab=tab_1
21. Bilson A, Talia A. Bruises in pre-mobile infants: a contested area of research, policy and practice. Pract Soc Work Action. 2022;35(4):281–96. doi:10.1080/09503153.2022.2140132
22. Department of Health. Maternal and Child Health Service practice guidelines [Internet]. 2019 [cited 2025 Aug 5]. Available from: https://www.health.vic.gov.au/publications/maternal-and-child-health-service-practice-guidelines
23. Johnson E, Jones A, Maguire SL. Bruising—the most common injury in physical child abuse. Paediatr Child Health. 2021;31(11):403–9.
24. City of Hume. Clinical Guideline. Bruising in the Immobile Infant. 2022.
25. Royal Children’s Hospital; 2021 [cited 2025 Aug 6]. Available from: https://www.rch.org.au/clinicalguide/guideline_index/Child_Abuse_Guideline/
26. Victorian Association of Maternal and Child Health Nurses (VAMCHN). Standards of Practice for Maternal and Child Health Nurses in Victoria [Internet]. Melbourne (AU): VAMCHN; 2024 [cited 2025 Aug 5]
27. Municipal Association of Victoria. Practice Note 1/June 2016: Learnings from the inquest of the Death of Baby D [Internet]. Melbourne (AU): Municipal Association of Victoria; 2016 [cited 2025 Aug 6]. Available from: https://www.mav.asn.au/__data/assets/word_doc/0019/23356/Practice-Note-1-Learnings-from-the-March-2016-Coronial-Investigation-into-the-death-of-Baby-D.docx