Abbreviations
- EBM - Expressed breast milk
- ED – Emergency Department
- EMCH – Enhanced Maternal and Child Health
- KAS – Key Ages and Stages
- MCHN – Maternal and Child Health Nurse
Definitions
- Faltering growth - (previously called ‘failure to thrive’) is widely used to refer to a slower rate of weight gain in childhood than expected for age and gender. The term faltering growth is preferred as periods of slow growth may represent temporary variation from the expected pattern and the word ‘failure’ may be seen as pejorative.
- Centile space - the space between adjacent centile lines on the World Health Organisation (WHO) and Centres for Disease Control and Prevention (CDC) growth charts.1,2
- Poor Growth - weight and / or length tracking downwards on percentiles.3
- Weight flattening - static weight gain pattern.
- Weight faltering - slower rate of weight gain than expected for age and gender.4,5
Background
- Faltering growth describes a child or infant whose current weight, or rate of weight gain is significantly below that expected for age and gender, or if weight has dropped ≥2 major percentile lines.
- Faltering growth may indicate inadequate growth for health and development and should trigger a medical and psychosocial assessment.
- There is not always an underlying pathological cause for faltering growth.
- Length and head circumference are often initially preserved in cases of faltering growth but may be affected if severe or prolonged insufficient nutrition.
| Causes of faltering growth | Examples |
|---|---|
| Inadequate caloric intake/retention |
|
| Psychosocial factors |
|
| Inadequate absorption |
|
| Excessive caloric utilisation |
|
| Other Medical Causes |
|
Assessment
Obtain and consider - maternal, perinatal, and postnatal histories
Intake:
- Breast/bottle/cup/spoon, number and volume/duration of feeds per 24-hour period, breast milk supply, formula type and preparation.
- Solids - age commenced, composition, number and quantity of meals and snacks.
- Milk intake per 24hr period in toddlers.
Output:
- Vomiting, stool, urine output, other losses (e.g. stoma) considering smell, colour, texture, amount, frequency.
- Any identified triggers to increased output. (e.g. specific food)
Food behaviour and dietary practices:
- Acceptance of food. (or parents feeling need to coerce/distract)
- Mealtime set-up and duration.
- Dietary restrictions. (see causes of faltering growth table below)
Past history:
- Chronic and current illness, recurrent infections.
Family growth:
- Pattern of weight gain and growth in other family members.
- Mid parental height. (an estimate of a child's adult height, calculated by averaging the parents' heights and adding or subtracting 13 cm)
Family psychosocial assessment:
- Signs of family vulnerability.
- Caregiver and child interactions.
- Be aware of risk factors for infants at risk of abuse or neglect. (see causes of faltering growth table)
Examination and full physical assessment:
- A general and holistic observational review of the infant is the most useful part of the assessment.
- Does the child appear in proportion and well, or do they look unwell? Significant malnutrition or illness.
- Hydration: significant dehydration. E.g. lethargic, irritable, increased respiratory rate, sunken eyes and fontanelle, dry mucous membranes, decreased skin turgor.
Signs of underlying systemic diagnosis
- Pattern of growth:
- plot serial measurements of weight, height and head circumference
- consider/exclude plotting errors
- clarify circumstances at times where growth trajectory changed e.g. introduction of solids, illness.
- Mid-parental height.
- Muscle bulk (buttocks), subcutaneous fat stores (thighs), skin, hair, gums, eyes and nails.
- Review muscle tone, observe for the presence of excessive or weak cry
- Oral assessment e.g. cleft palate, oral thrush, tongue tie (consider scope)
- Developmental level, caregiver-child interactions, signs of abuse or neglect
- Observe feed. (breastfeed, bottle feed, and/or solids meal)
Ensure growth is adequate
- Growth charts
- <2 years of age: WHO growth standards. Correct for prematurity (<37 weeks) until 2 years old
- ≥2 years of age: CDC growth reference charts
- use specific growth charts. (e.g. Down, Turner syndrome) where appropriate
Growth chart interpretation
- In the first few months of life, a healthy baby who is gaining weight may cross and track along a lower centile than that of their birth weight.
- Length and head circumference are usually initially preserved in cases of faltering growth but may be affected if severe or prolonged insufficient nutrition, if this is observed the child requires medical review.
- Children with isolated less than 3rd percentile weight-for-age, but with typical neurodevelopmental progress and no red flags on clinical assessment may still be within normal limits of growth.
- these children should be monitored over time and may not need extensive investigation.
- A drop in percentiles may be observed when switching from WHO to CDC charts
- this is usually due to differences in the charts rather than representing a true change in growth pattern.
Average growth
- Although the use of a growth chart is the most accurate indication of overall growth the use of average weekly weight gain for children who are followed up at frequent intervals may be required.
- The rate of weight gain per week is variable.
The table below is a guide to the expected average weight gain per week. (it is not the minimally acceptable weight gain)
| INFANT (0 month to 12 months) 6,3 |
|
|---|---|
| Infants birth – 3 months | 20-30gms / day or 150-200gms / week |
| Infants 3 - 6 months | 15-20gms / day or 100-150gms / week |
| Infants 6 - 12 months | 10-13gms / day or 70-90gms / week |
CHILD (12 months and over) |
|
|---|---|
Infants 12 months - 2 years | 2-3 kgs per year (~ 40-50gms per week) |
Children 2 years - 5 years | 2 kgs per year (~ 40gms per week) |
More information on how to interpret child growth can be found at:
Growth charts | Royal Children's Hospital
Growth and Growth Charts | Australian Paediatric Endocrine Group
The frequency on how to measure is based upon investigation of cause
NOTE: If there are concerns about faltering growth, weight should be measured at appropriate intervals taking account of factors such as age and the level of concern but usually no more often than:
- weekly between 1 and 6 months old
- Fortnightly between 6 and 12 months old
- Monthly from 1 year old.
Weight monitoring every 1-4 weeks is usually sufficient in infants, depending on the level of concern.3,7
Management
A multi-disciplinary team approach is highly recommended. Professionals may include:
- maternal and child health nurse and/or lactation consultant
- general practitioner (GP), paediatrician
- dietician, speech pathologist, multidisciplinary feeding clinic
- psychologist, infant mental health clinician
- social worker or child protection services
- early parenting centre.
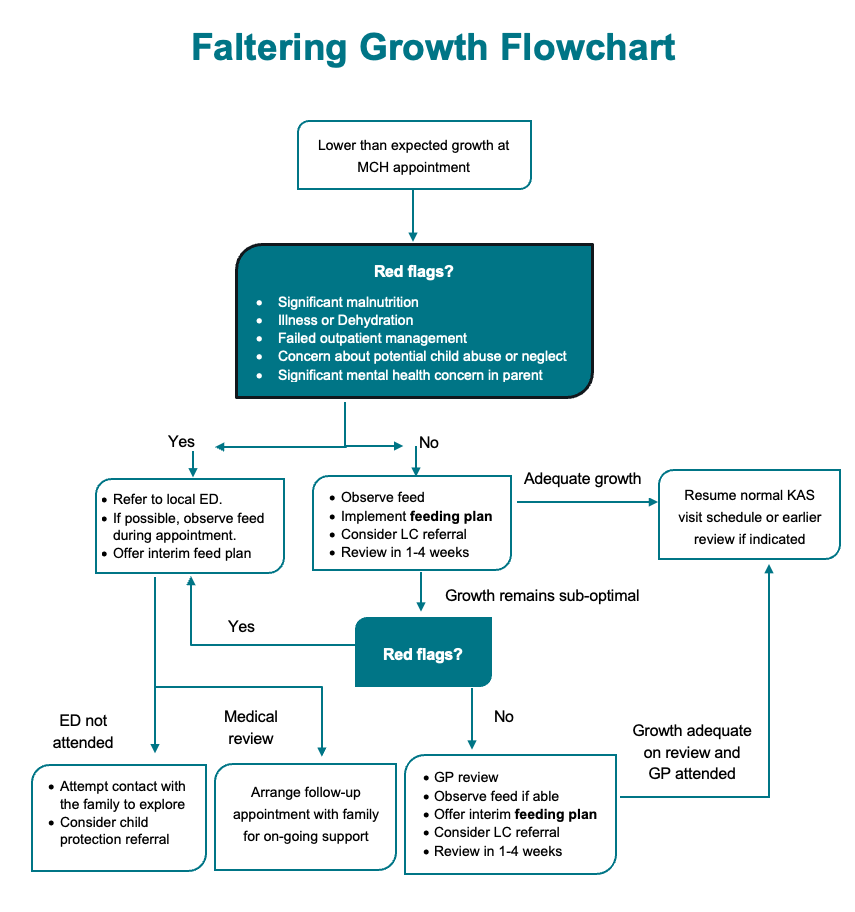
Promptly arrange acute paediatric referral if:
- signs of dehydration, illness or severe malnutrition.
- failed outpatient management
- signs of abuse or neglect
- significant mental health concerns in carer
- for further assessment of feeding technique, parent-child interaction and involvement of a multidisciplinary team
- significant faltering growth persisting despite intervention.
For exclusively or partially breastfed infants suspected of sub-optimal intake with no paediatric red flag concerns:
- observe a whole breastfeed, where possible and practicable
- provide advice on attachment, positioning, feeding cues, increasing supply, responsive feeding principles, red flags requiring medical attention
- consider the use of switch feeding (offering each breast twice, changing sides when the baby is no longer observed to be swallowing regularly) and breast compressions (gently compressing the breast) to increase milk flow.
- consider introducing complementary feeds using expressed breast milk or formula if required, provide education to the caregiver regarding paced bottle feeding and responsive feeding techniques
- implement feeding plan in consultation with carer
- refer to LC or breastfeeding services if appropriate
- consider GP review of appropriateness for galactagogue use and possible risk factors for low supply e.g. retained products.
For exclusively or partially bottle-fed infants suspected of suboptimal intake with no acute paediatric red flag concerns:
- observe a bottle feed, looking for signs of feeding difficulties that may require specialist input such as aspiration or feeding aversion
- provide guidance to the caregiver regarding appropriate paced and responsive bottle-feeding technique
- for formula fed babies, ensure formula is being prepared and stored appropriately
- ensure milk volume intake is appropriate
- implement or modify feeding plan in conjunction with the parent if required.
For the older infant/child who has commenced solid foods:
- observe a mealtime (if not practical to do this within the clinic environment consider telehealth review)
- provide advice on feeding cues, responsive feeding principles and age-appropriate calorie dense foods
- implement or modify feeding plan in conjunction with the parent
- consider any financial difficulties that may be impacting access to food.
On-going care
- organise follow up review as per recommended age table
- if there is no appointment available within the appropriate time frame for follow-up, a KAS appointment for an older child should be re-scheduled to allow for the follow-up appointment, if this is not possible the MCHN should escalate their concerns to their team leader/coordinator
- on follow up review if the growth tracks appropriately, review and modify feeding plan as appropriate and return to usual schedule of KAS consults
- if growth continues to falter for a subsequent visit despite appropriate implementation of and adherence to the feeding plan, refer for a medical review with GP and continue MCH follow up review as per recommended age table in consultation with parent
- in conjunction, also consider referral to feeding support services such as lactation consultant, dietician or speech pathologists
- if follow up appointments are not attended, action should be taken to ascertain the wellbeing of the child. Refer to Child Protection if considered to be at risk.
Follow-up
- inform caregiver of concerns
- frequency of follow up will depend on the child's weight, age and psychosocial circumstances
- recommend follow-up review appointment in:
- 1 week (infant aged 4 weeks to 6 months old)
- 2 weeks (infant aged between 6 and 12 months old)
- 1 month (older child >12 months)
- if weight continues to be static or falling at next review despite intervention —refer to GP for medical review, or local Paediatric ED if any red flags (see above) for further investigation
- if the Infant has gained weight at the next assessment, then adjust feeding plan as needed and weigh again in:
- 1-4 weeks (infant aged 4 weeks to 6 months old)
- 2-4 weeks (infant aged between 6 and 12 months old)
- 1-2 months (older child >12 months)
- if weight continues to increase appropriately, further modify or cease feeding plan and additional growth checks. Return to routine KAS appointments unless otherwise indicated.
Referrals
Refer family to present in person to their local paediatric ED same day if:
- signs of dehydration, illness or severe malnutrition.
- signs of abuse or neglect
- significant mental health concerns in carer
- for further assessment of feeding technique, parent-child interaction and involvement of a multidisciplinary team
- significant faltering growth persisting despite intervention.
If unsure whether the child needs to present to their local ED, consider use of the Victorian Virtual ED for secondary consult prior to presenting to a face-to-face ED, this can be done by the family on their own or with the MCHN present.
If the family does not present to the ED as planned, consider a referral to child protection.
Refer to GP if:
- faltering growth continues despite initial management amendments/ feeding plan implementation
- faltering growth identified at 2 consecutive appointments
- requiring support for any identified red flags.
If unable to organise a timely GP appointment, or if required, consider secondary consultation with the Victorian Virtual Specialist Clinics General Paediatric service, this should be arranged as a co-consult with the family and the MCHN both present for the appointment.
Consider community-based referral supports in conjunction with any required medical review:
- lactation support services
- allied health services
- perinatal or infant mental health services
- early parenting centre programs
- social work
- EMCH.
Information for health professionals
Breastfeeding Support and Guidelines – RCH Nursing Guideline Breastfeeding Support and Promotion
Slow Weight Gain Clinical Practice Guideline
SCV Breastfeeding for Neonates
Information for families
Pregnancy Birth and Baby How Your Baby Gains Weight
Pregnancy Birth and Baby Slow Weight Gain
Breastfeeding Kids Health Info
Raising Childrens Network Child Growth Charts 0-2 years
Growth Charts for Children Better Health Channel
Nurturing Young Children Through Responsive Feeding WHO
How to tell if your child is sick
References
- World Health Organization. WHO child growth standards: growth velocity based on weight, length and head circumference: methods and development. Geneva: World Health Organization; 2009. Available from: https://iris.who.int/handle/10665/44026
- Centers for Disease Control and Prevention. CDC growth charts [Internet]. Atlanta (GA): National Center for Health Statistics; [updated 2024 Sep 2; cited 2025 Sep 9]. Available from: https://www.cdc.gov/growthcharts/cdc-growth-charts.htm
- The Royal Children's Hospital Melbourne. Clinical practice guidelines: slow weight gain [Internet]. Melbourne (AU): The Royal Children's Hospital; 2021 [cited 2025 Sep 9]. Available from: https://www.rch.org.au/clinicalguide/guideline_index/Slow_weight_gain/
- National Institute for Health and Care Excellence (NICE). Faltering growth: recognition and management of faltering growth in children. NICE guideline [NG75]. 2017 Sep 27 [cited 2025 Aug 12]. Available from: https://www.nice.org.uk/guidance/ng75
- Dean E. Faltering growth [Internet]. Nurs Child Young People. 2017 Jun 12;29(5):11. Available from: https://doi.org/10.7748/ncyp.29.5.11.s11 [cited 2025 Sep 8].
- National Health and Medical Research Council. Infant Feeding Guidelines: Information for Health Workers. Canberra: National Health and Medical Research Council; 2012. (Publication no. N56). ISBN: 1864965665. Available from: https://www.nhmrc.gov.au/about-us/publications/infant-feeding-guidelines-information-health-workers
- National Institute for Health and Care Excellence (NICE). Postnatal care. NICE guideline [NG194]. 2021 Apr 20 [cited 2025 Aug 12]. Available from: https://www.nice.org.uk/guidance/ng194